Why a Campaign for a National Care and Support Service (NCSS) would still promote oppressive practice
 Bob Williams-Findlay writes: The following piece reflects my own view and is not necessarily the representative of the views held by either the Reclaiming Our Futures Alliance or Left Unity. Noting I am being critical of the six principles the Social Health Association and Keep Our NHS Public should not be taken as an indication that I also reject the urgent need for a campaign around the crisis state of Social Care (sic) or the need to tap into the anger generated by the government’s policies before and during the pandemic. I believe these principles are unacceptable as they currently stand because they perpetuate a model of service delivery that is totally bankrupt and oppressive.
Bob Williams-Findlay writes: The following piece reflects my own view and is not necessarily the representative of the views held by either the Reclaiming Our Futures Alliance or Left Unity. Noting I am being critical of the six principles the Social Health Association and Keep Our NHS Public should not be taken as an indication that I also reject the urgent need for a campaign around the crisis state of Social Care (sic) or the need to tap into the anger generated by the government’s policies before and during the pandemic. I believe these principles are unacceptable as they currently stand because they perpetuate a model of service delivery that is totally bankrupt and oppressive.
Immediately below are the six principles the Social Health Association and Keep Our NHS Public have developed independent of consultation with ROFA or other Disabled people’s led organisations to shape a new campaign. I have stated previously that there are certain aspects of the principles I see as of value, but the main thrust, I totally reject. I will briefly explain why in due course.
Campaign for a National Care and Support Service (NCSS)
In the aftermath of World War II, people in the UK demanded a National Health Service that would provide comprehensive health care to those who need it, free at the point of delivery.
In the face of the near collapse of social care services following years of austerity, profiteering by private companies and the devastation wreaked by Covid-19, we demand the Government establish a National Care and Support Service (NCSS) with the following principles:
1. A National Care and Support Service (NCSS):
The Government shall have responsibility for and duty to provide a National Care and Support Service (NCSS) to provide care, support and independent living as set out in the Care Act 2014 and Article 19 of the UN Convention on rights of disabled people.
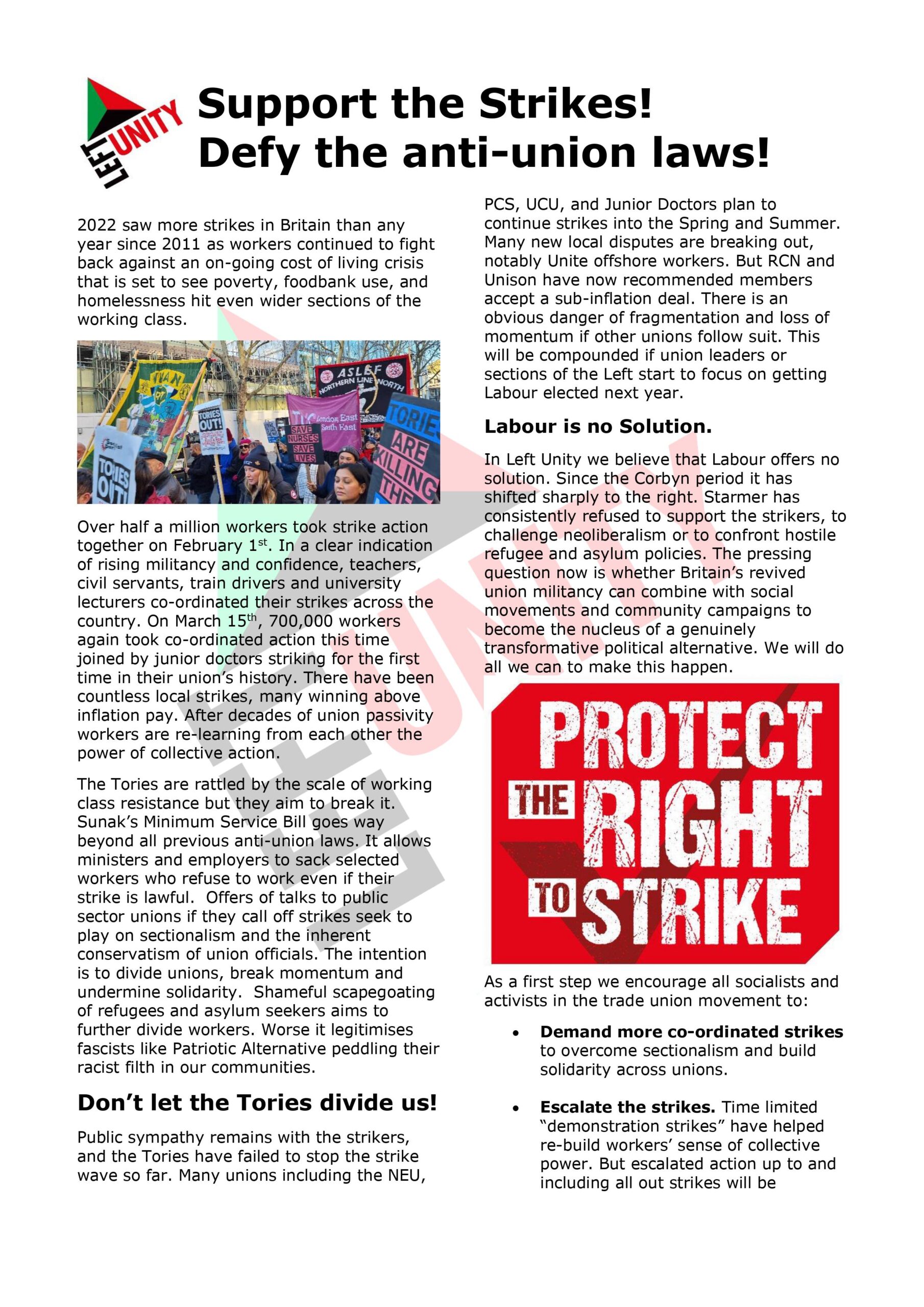
2. Fully funded through progressive taxation, free at the point of need and fully available to everyone living in this country.
3. Publicly provided and publicly accountable:
The NCSS will have overall responsibility for publicly provided care homes and care providers and, where appropriate, for the supervision of not-for-profit organisations funded through grants allocated by the NCSS. All provision will deliver to NCSS national standards. The market in social care, including the profiteering that exists within sections of social care, will be ended.
4. Nationally organised, locally delivered:
The Government will be responsible for delivery by the NCSS, of democratically run services, designed and delivered locally and co-productively, involving service users and carers, local authorities and the NHS.
5. Support for carers:
The NCSS will ensure that informal and family carers are well supported, can have a full life of their own and are not expected to provide more care than they willingly offer.
6. National NCSS workforce strategy fit for purpose:
The NCSS services and standards will be underpinned by a workforce who have appropriate training, qualifications, career structure, pay and conditions to reflect the skills required to provide support and care services worthy of a decent society.
My position is clear: anything established within a framework that builds on or takes from the traditional way older and Disabled people have been both seen and treated is unacceptable. The dominance of the notion of “Care” within service provision has a long history back to the 14th century Poor Laws and played a major role in the creation and maintenance of Disabled people’s social oppression. The prominent position of “Care” in service provision feeds disablism, ageism and sexism.
I have outlined elsewhere how the ideologically oppressive narratives around “Care” creates power dynamics of ‘them’ and ‘us’. Byrony Shannon’s Blog on the word “Care” captures very well why SHA and KONP are missing the bigger picture:
The narrative of ‘care’
Ultimately care is about people. Us. All of us. But the narrative of care is about them. Others. ‘The vulnerable’ who need to be cared for, in another setting. In another sector. A bureaucratic system, where decisions are made for and about ‘service users’, not by or with people.
The focus on care invariably concentrates on ‘personal care’: managing and maintaining nutrition, personal hygiene, toileting needs – and too often this becomes the focus of care plans. The life and limb care to ensure survival.
It also perpetuates the medical model – focusing on what’s wrong, grouping and labelling people by diagnosis and condition, prescribing solutions and looking after people in institutions. A narrative that convinces many that the answer to the ‘care crisis’ lies in further integration with health.
Prior to COVID-19, social care had little profile, largely absent from public consciousness and political discourse. In the early days and weeks of the UK Government’s response to the pandemic, the sector’s subservient relationship with health was apparent as care homes bore the brunt of the ‘protect the NHS’ message. And as the current crisis evolves, the true cost of those early political decisions is becoming increasingly, and heartbreakingly, apparent to those of us working in or closely with care homes, or who have relatives or friends living, and dying, in them.
Putting social back in to care
The Government’s badge says ‘CARE’. But what happened to the social element? OK so yes, it’s often absent from care plans which focus on personal care at the expense of personal relationships. And it’s increasingly absent from social work teams, as we hot-desk and work from home. But surely one of the glaring messages from the last few months is that we need each other – our families and friends and neighbours and colleagues. So many of us have experienced a loss of connection. An element of isolation. A feeling of loneliness. The absence of touch. The lack of hugs. We’re all hugely aware that there’s so much more to life than meeting our basic needs for food and drink, clothing, shelter and safety. We need to be part of a bigger whole. We need to belong. We need to love, and to be loved in return.”
Where I have a problem with Byrony, and the principles for the campaign, is here:
“Ultimately care is about people. Us. All of us. But the narrative of care is about them. Others. ‘The vulnerable’ who need to be cared for, in another setting. In another sector. A bureaucratic system, where decisions are made for and about ‘service users’, not by or with people.”
The narrative of care articulates the practice of disablism; where “care” is NOT about people of equal value, but ‘burdens’ on society as a whole. If the narrative of care is about them, who then are subjected to “Othering”; their status as ‘people’ becomes diminished or removed altogether. So currently, it is false to say that in the end ‘care is about people’, because our system works against collective support and ‘common good’. In order to create the conditions whereby care is really about people, we must transform society, beginning with how we both see and treat older and disabled people. Perhaps this sounds strange, but this requires ending the oppressive notion of “Care” within society policy. This is why the idea of a new National Care and Support Service is unacceptable to people like me. I believe it will result in having the same toxic poison, just a different bottle; it is impossible to ‘reclaim Social Care’.
We need a fresh start that puts human dignity and respect at its heart. The focus has to be ‘independent living’, however as the European Network for Independent Living explains: ‘IL does not mean being independent from other persons, but having the freedom of choice and control over one’s own life and lifestyle.’
This is why the principles outlined by SHA/KONP contain the words ‘independent living’ but without any understanding or commitment to what it really is all about.
ENIL defines it as:
Independent living is the daily demonstration of human rights-based disability policies. Independent living is possible through the combination of various environmental and individual factors that allow disabled people to have control over their own lives. This includes the opportunity to make real choices and decisions regarding where to live, with whom to live and how to live. Services must be available, accessible to all and provided on the basis of equal opportunity, free and informed consent and allowing disabled people flexibility in our daily life. Independent living requires that the built environment, transport and information are accessible, that there is availability of technical aids, access to personal assistance and/or community-based services. It is necessary to point out that independent living is for all disabled persons, regardless of the gender, age and the level of their support needs.
Now consider the first principle:
The Government shall have responsibility for and duty to provide a National Care and Support Service (NCSS) to provide care, support and independent living as set out in the Care Act 2014 and Article 19 of the UN Convention on rights of disabled people.
Where is the emphasis and weight here? Talking about ‘as set out in the Care Act 2014 and Article 19 of the UN Convention on rights of disabled people’ shows their total ignorance of what is at stake. This ignorance is further evidenced by this principle:
‘The NCSS will have overall responsibility for publicly provided care homes and care providers and, where appropriate, for the supervision of not-for-profit organisations funded through grants allocated by the NCSS. All provision will deliver to NCSS national standards.’ What this principle offers is public ownership rather than privately owned oppressive shit! I stand with ENIL on this fundamental human right:
Deinstitutionalisation is a political and a social process, which provides for the shift from institutional care and other isolating and segregating settings to independent living. Effective deinstitutionalisation occurs when a person placed in an institution is given the opportunity to become a full citizen and to take control of his/her life (if necessary, with support). Essential to the process of deinstitutionalisation is the provision of affordable and accessible housing in the community, access to public services, personal assistance, and peer support. Deinstitutionalisation is also about preventing institutionalisation in the future; ensuring that children are able to grow up with their families and alongside neighbours and friends in the community, instead of being segregated in institutional care.
SHA/KONP have focused on ownership, standards and resources within institutional care and other isolating and segregating settings without even questioning why they exist or if they are actually what is needed.
The fourth principle also demonstrates a lack of understanding of disablism at work:
‘The Government will be responsible for delivery by the NCSS, of democratically run services, designed and delivered locally and co-productively, involving service users and carers, local authorities and the NHS.’
What does ‘co-productively, involving service users and carers, local authorities and the NHS’ actually mean as a principle? There are only a handful of good examples of ‘co-production’ where the leadership is NOT the nondisabled professionals. Sorry, ‘involving’ is a word our oppressors employ whilst controlling us!
And the final principle I totally reject is this one:
‘The NCSS will ensure that informal and family carers are well supported, can have a full life of their own and are not expected to provide more care than they willingly offer.’
Where does one start with this oppressive mindset? We need to understand the contexts in which informal and family takes place; again the question of choice and control, the need to point the finger at the way the system fosters ‘dependency’ and forced responsibilities; not collude in the continued exploitation and oppression. The fact that SHA/KONP can’t see an issue with this ideologically oppressive constructed principle should lead to people asking what kind of mindset are these ignorant people working within? This principle is degrading to both people who give and receive support
A National Independent Living Support Service would work to ensure independent living from a holistic perspective, therefore EVERYONE involved would be considered as having rights, especially the right not to be socially restricted, be that a child willing to support a disabled parent or an older parent with a adult disabled person still at home. SHA/KONP uses ‘care’ as a disablist disempowering notion – this is why I see them as part of the problem, not the key to a better future.
Left Unity is active in movements and campaigns across the left, working to create an alternative to the main political parties.
About Left Unity
Read our manifesto
Left Unity is a member of the European Left Party. ![]()
Read the European Left Manifesto
ACTIVIST CALENDAR
Events and protests from around the movement, and local Left Unity meetings.
Saturday 19th July: End the Genocide – national march for Palestine
Join us to tell the government to end the genocide; stop arming Israel; and stop starving Gaza!
Summer University, 11-13 July, in Paris
Peace, planet, people: our common struggle
The EL’s annual summer university is taking place in Paris.
More events »
GET UPDATES
Sign up to the Left Unity email newsletter.
CAMPAIGNING MATERIALS
Get the latest Left Unity resources.