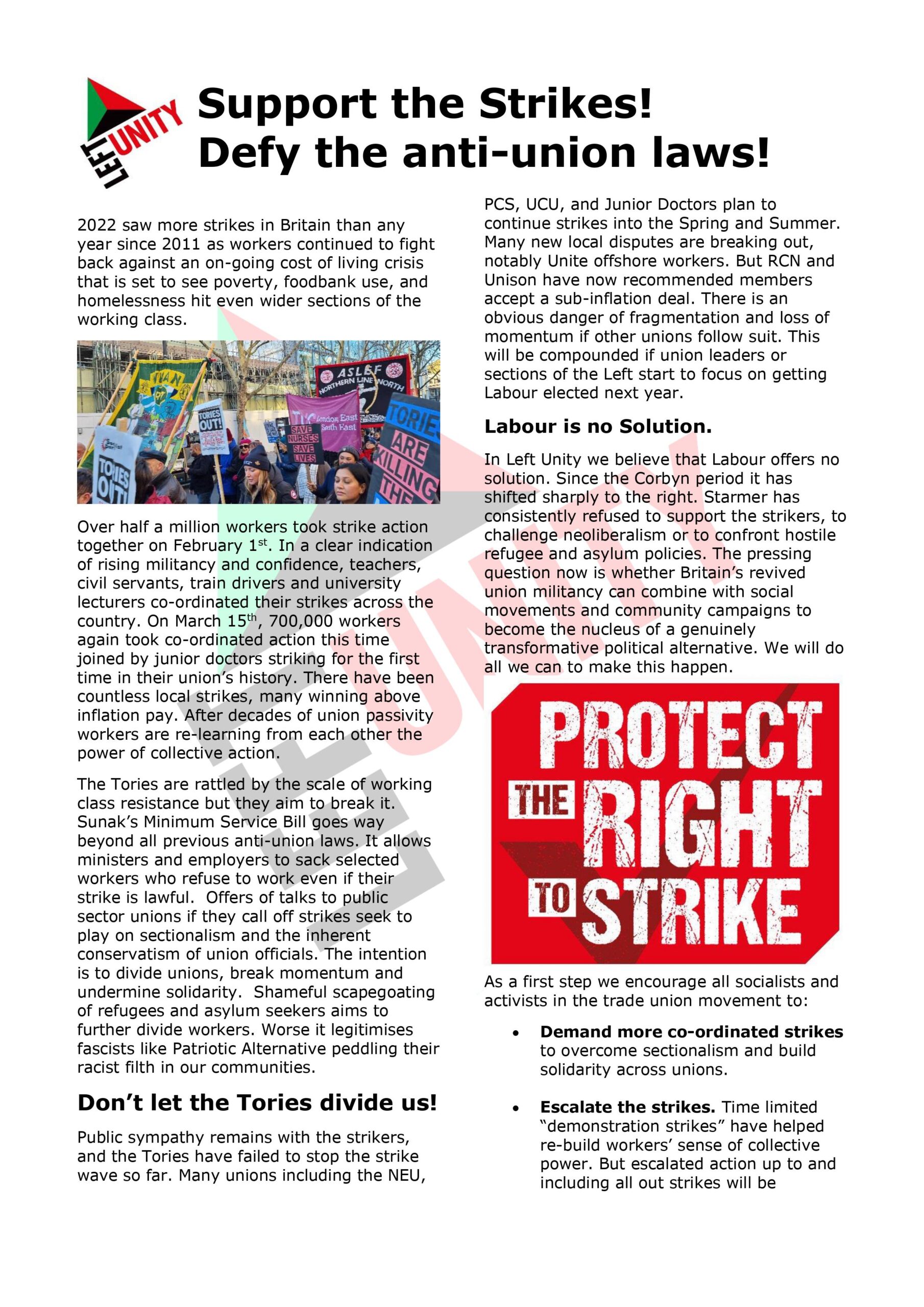
Vote for the NHS this week, Vote Labour!
Felicity Dowling draws parallels with the US health system and argues that defence of the NHS is a crucial reason to vote Labour.
The National Health Service, founded in the aftermath of an unprecedented war and the 1945 Labour victory, is a truly valued institution. It was founded to be free at the point of need, publicly provided, funded from taxation, and a universal service. It is now being carved up to make money for big corporations, and services are being run down.
There are many warrior groups defending the NHS in this election and their work will continue.On a Facebook group called Pride in the Port (Ellesmere Port), someone recently commented favourably about the US health care system, as a reason not to vote Labour. So I asked friends and family from the USA for information on how the US system worked for them, this is just a sample of their replies.
From John R:
“The money is a major issue, but so is the stress and insecurity in the US system.
This is just off the top of my head. The main point is this: Yes, if you have unlimited resources you can get better health care in the US than anywhere else. That is probably what’s pointed to when they talk in Britain about the “wonderful” health care system here. But, that’s strictly for those with the money, and I’m talking about many millions. For the rest, wait times, everything else is rotten”.
From another friend, this time in the UK:
“I’m diabetic and my diabetic friends in the US have to pay up to $3,000 a month for insulin and blood testing equipment. Insurance doesn’t always cover all the costs and they are often denied insurance for blood glucose monitoring, insulin pumps and insulin itself.”
Another UK friend wrote:
“My son spent last summer in the US, coaching football. One drunken evening he stuck a knife through his palm. The care was good; they stitched him up, dressed the wound and gave him some antibiotics. A few days later, he went back and they re-dressed the wound. The bill for that was £12,000. Luckily, he was insured. There’s a lot of money to be made from private healthcare.”
Sonja, in the US, sent me this:
“I pay almost $400 a month for private insurance. That is almost 25% of my monthly net income. Still, I had knee surgery just recently and am stuck now with a bill of $7,500. I knew my deductable was $ 2,500, but apparently, I have another co-payment of 30% (for outpatient surgery?), I am not sure. Anyway, a high amount of money to pay (almost 1/3 of my annual income) for somebody who pays already a lot for insurance. The private insurance system in the US sucks. I can’t believe anybody in Europe would see it as a good example (for anything)…”
My sister in law wrote:
“It’s not only the costs. Last year a friend became very unwell and I took her to the after-hours medical centre. After waiting her turn she was informed that she would have to go to another similar after-hours medical centre across town, because the two centres accepted different types of insurance. The paperwork she had to complete before being seen was quite a few pages long. It did not help matters that she was from another state. I couldn’t believe how convoluted the system has become”.
Yet another friend wrote:
“In addition to the paperwork, there is also the stress. My cousin in New York had a hip operation at the same time as my Dad was in ICU in London. The former had to worry about how she was going to pay the bill when she got out, while my Dad had only to worry about getting better and the inconvenience of the tubes and wires that were attached to him. No bills, means less stress, means better health outcomes! Duh!”
Another family member commented:
“Healthcare access in the United States is a disgrace. I am a provider as well as a patient like everyone else. For providers, it’s stupidly complex. We have to waste so much time worrying about the different insurance companies, different policies, stupid amounts of paperwork, instead of taking care of our patients. When it comes to accessing medical care, Obamacare allowed many of us who couldn’t get an affordable policy because of our age and/or pre-existing conditions to get into the “market”. But, compared to the rest of the developed world, our system is cruel and horribly expensive. I could go on and on. It’s an embarrassment that we don’t have universal coverage. A little known fact about the US: there is no cap on how much a person on Medicare (the universal coverage system we have for people over 65, thanks to President Lyndon B. Johnson) will have to pay for a catastrophic injury or illness. By definition, getting older means higher medical costs for most people. Many people who reach the last part of their lives end up spending every penny of their savings on illness – because even though we have Medicare, there are still “co-pays” and “deductibles”. Healthcare is never free in the United States. Once they have exhausted all of that, if they need skilled nursing care, they will be covered by the safety net program called Medicaid. But, you only get that if you are basically bankrupt. Donald Trump wants to drastically cut Medicaid. Many ignorant people think that Medicaid is for lazy young people who don’t want to work. The truth is nearly all of it goes toward elderly people who are in poverty and only have Medicaid to rely on for a nursing home. Without Medicaid, our elderly would literally be thrown into the streets.
If you’re over 65 years of age, Medicare will help pay the cost. As mentioned above, Medicaid will pay for nursing home care for people who are destitute. Medicare covers up to 90 days in a nursing home. If under age 65 and no insurance, all medical costs are the responsibility of the patient. They are totally exposed.”
A friend of my sister in law commented:
“Here’s one example: there are 13.5 million people in California who are on Medi-Cal, which is the government-sponsored health insurance program for those who don’t earn enough to be able to afford private health insurance. This program is a step in the direction towards what Britain has, not a step away from it. One problem is that many doctors in the state won’t accept Medi-Cal patients because the payments are so low. There is a similar issue for private insurance: except for the premium insurance plans, which cost an arm and a leg, the lower cost plans often limit the coverage so that it’s difficult to find a doctor in your area, especially specialist doctors.”
Another friend of the family wrote:
“….. asked me to relay my experience many years ago, when I had no health care coverage. I had just been dumped off my parents’ coverage, at age 22 I think, and my position at the time didn’t provide me with any health care coverage. I ended up in the local hospital with a bout of kidney stones. I was in the hospital for almost a week, when they realized that I needed to go over to a hospital in Eugene, Oregon, to have a stone removed. I was in that hospital for about 3 days after the stone removal. With around 10 days in the hospital, the doctors’ fees from the first hospital, the surgeon’s fees from Sacred Heart Hospital, and fees for consulting physicians, I ended up with about $5,000-$6,000 in medical bills. Doesn’t sound like much in today’s climate, but in 1984 it was a lot of money for a graduate student. It took us just shy of 10 years to pay that off, a little bit at a time. We even had some issues with the IRS about why we were unable to pay some taxes and once they added up all our monthly bills, they figured out that we were maxed out on our monthly income pretty much due to my medical bills and my husband’s student loan debt! Today that amount would probably be closer to about $15,000. But I would venture to guess that the medical costs today would probably be closer to $30,000. Our health care system here in the US is atrocious and will only be made worse by the AHCA!”
Suzanne commented:
“And when you do have private insurance coverage, it’s still not anything like “free at the point of need”. My mother paid for an “enhanced” health insurance policy over the course of her entire working life, right up to the time of her death at 95. She still had co-pay for medicines, and would ask me to help her put eye drops in when I visited, as each “drop” cost $25 and her hand wasn’t steady! In the last 6 months of her life she was still at home, but needed more care than the 10 hours a week she was paying for from her insurance. When I tried to help her put more in place, she was anxious that she’d run out of money before she would die if she had to spend more – a worry I thought was irrational, until I looked at the policy details. It was, indeed, as she had said: a finite sum of money. And when it was used up, tough bananas. In addition, the insurance company would pay for her to be in residential care, but limited how many hours of help she could have in her home. And if she required specialist help of any kind, it was assessed ATOS-style, i.e. when she had an eye operation and had to lie face-down for several days, the question asked was “if food is put before you, can you feed yourself?”, not, “are you able to prepare food for yourself and then feed yourself?” And so, she was denied the help she really needed then.
And she specifically took out cover so that someone might be able to live with her to give her full-time help, but it was so stringent that she never got to use that aspect.”
John reported that:
“There’s a similar problem for Medicare, which is the government-sponsored health insurance for people over 67. Most doctors accept Medicare, but I think the payments must be lower than what private insurance pays. The reason I suspect that is this: as somebody on Medicare, I’ve called some specialists for an appointment and have been told I’d have to wait over a month for my appointment. But my wife, who isn’t on Medicare, was able to get an appointment with the same doctor for herself within a week! What I suspect happens is that the doctors limit the number of Medicare patients they accept.
“And then there’s those who choose to go uninsured. This is very risky because ALL doctors and ALL hospitals charge the uninsured over double what they charge the insurance companies. I’ve heard of people from out of the US who stayed in the hospital overnight for some relatively minor problem and were charged over $10,000.”
Compare all of this to Britain: a few years ago I had a medical emergency while I was visiting London. I went to an emergency room, was seen in an hour (which is a short waiting time in a hospital here) was given the drugs I needed and was out of there. Total cost: my taxi ride to and from the hospital. The same here would have been probably a couple of thousand dollars.
Jono commented: “are you aware that the advertising of family history, genealogy sites and DNA testing for ancestry is funded by groups with links to health insurance. Predicting the likelihood of incidence? Setting the price list to match your genetic propensity!
Someone else told me the wrist devices linked to your phone similarly share to health insurance companies.”
A comment (not to do with my post) on how families in the Manchester tragedy would have fared in the US went viral. It came from Hannah Middlebrook (a warrior for social justice in Tulsa, Oklahoma, I checked it with a friend) Hannah said:
“I’ve neglected to give you any US healthcare information these last few days. Sorry about that. But after reading this morning’s terrible news, it struck me my friends in the UK need to hear something many Brits may not have considered.
If the Manchester Arena bombing had happened in the US, every family with a dead or injured member would begin receiving bills in the coming days. Parents who lost their children would get a detailed and unadorned list of services provided by the medics that tried to save their relations’ lives. And they would be expected to start making payments immediately.
While they mourned heart-breaking losses, American families would be billed for the ambulance rides, morphine, CPR, anesthesia. They would be expected to pony up for surgeries that were unsuccessful, medication that didn’t work, and the time the anesthesiologist spent trying to keep their children comfortable during major procedures. They would continue to receive those bills for month upon month after the death of their children.
Many families would set up GoFundMe accounts to pay for the medical expenses of their deceased child. The bills would run in to the hundreds of thousands, so even the best-funded account would only pay a fraction. The parents might have to sell their homes while trying to wrap their minds around the needless loss of their children. Ultimately, many would declare bankruptcy: who has time to pore over bills, fight the constant inaccuracies, totalling hundreds or thousands of dollars, when they’re battling depression and anger?
“Think about that. It’s the kind of society you’re really signing up for when you vote for a party that wants to privatise your healthcare. Please don’t make that mistake.”
I checked this out with friends who commented:
“…the National Student post about health and the Manchester Arena bombing. She is correct except for those government-funded programs that are similar to Medicare for all. These are Medicaid and the Veterans Admin. health program where all costs are born by the government. Note Medicare is NOT Medicaid. Medicare has premiums, co-pays and deductibles.
Obama care expanded the number eligible for Medicaid, which is for low income people, while ‘Trumpcare’ proposes to remove 14 million people from Medicaid. By the way, my eldest step-daughter passed away on May 16 after three weeks in hospital, and yesterday we received a letter saying she will not owe anything because she is on Medicaid and if she does get billed to contact the hospital. P.S. in California Medicare is called Medi-Cal.”
There was much more.
A friend sent me this link https://newrepublic.com/article/142368/devastating-effects-dental-inequality-america from which one small part:
“But here’s an unfortunate rule in medical history, at least in the United States: the untreatable conditions of the past become the untreated tragedies of the present. Mary Otto’s heartrending and incisive book, Teeth, builds on her Washington Post story on Deamonte Driver, a black twelve-year-old from Maryland who “died of a toothache” in 2007. His life could have been saved, she wrote, if his family had insurance, or if they had not been stripped of Medicaid for a time when they were homeless, or if Maryland’s underfunded Medicaid program had provided adequate access to dentists. “By the time Deamonte’s own aching tooth got any attention,” Otto reported, “the bacteria from the abscess had spread to his brain.” Surgeries and no doubt much suffering followed, but it was too late.”
Suzanne sent me these links:
http://khn.org/news/unitedhealth-doctored-medicare-records-overbilled-u-s-by-1-billion-feds-claim/
and Alice sent me this: https://www.facebook.com/alice.kilroy/posts/10158807072285226?hc_location=ufi
and John yet another:
I send solidarity to all in the US who face such a system and who campaign to change it. The best way to support them is to defend our NHS.
In this election please vote for and campaign for the NHS, free at the point of need, publicly provided and not for profit, a universal service paid for from taxation.
We know many UK health institutions have been in contact with Kaiser Permanente a huge US provider: https://tompride.wordpress.com/2017/04/23/theresa-mays-secret-plans-to-replace-nhs-england-with-private-us-healthcare-system-kaiser-permanente/
We know the NHS has imposed an Accountable Care Organisations model similar to the US system in some areas, including where I live.
This is critical in these last vital days of the election campaign. Vote for the NHS. Defend the NHS after the election to support a Corbyn government or to defend our NHS in other ways.
Left Unity is active in movements and campaigns across the left, working to create an alternative to the main political parties.
About Left Unity
Read our manifesto
Left Unity is a member of the European Left Party. ![]()
Read the European Left Manifesto
ACTIVIST CALENDAR
Events and protests from around the movement, and local Left Unity meetings.
ongoing
Just Stop Oil – Slow Marches
Slow marches are still legal (so LOW RISK of arrest), and are extremely effective. The plan is to keep up the pressure on this ecocidal government to stop all new fossil fuel licences.
Saturday 27th April: national march for Palestine
National demonstration.
Ceasefire NOW! Stop the Genocide in Gaza: Assemble 12 noon Central London
Full details to follow
More events »
GET UPDATES
Sign up to the Left Unity email newsletter.
CAMPAIGNING MATERIALS
Get the latest Left Unity resources.