Draft policy statement on assisted dying/suicide, individual autonomy and the freedom to make choices
Bob Williams-Findlay introduces a draft statement from the Left Unity Disabled Members Caucus
After much debate within the LUDM Caucus we have produced a DRAFT POLICY STATEMENT ON ASSISTED DYING/SUICIDE, INDIVIDUAL AUTONOMY AND THE FREEDOM TO MAKE CHOICES. This is a very detailed exploration of key concepts and arguments followed by a proposed motion. Our Caucus believes there is an urgent need to discuss these issues within Left Unity with Rob Marris introducing a Private Members Bill on ‘Assisted Dying’ on the 11th September, 2015.
It is acknowledged by the LUDM Caucus that there’s a great deal of sympathy for people with terminal illness to have a legal right to assisted suicide, often branded as ‘dignity in death’, however this sympathy is often given without adequate consideration of what is actually being pushed for and the social implications involved. Many on the Left believe in individual autonomy, as do members of our Caucus, however a close examination of Marris’ Bill reveals that in reality the argument – this is about the freedom of choice – is bogus. The driving force behind this Bill is the desire to change the legal and social landscape.
People who are terminally ill are imprisoned by their conditions, according to Sir Patrick Stewart, President of Dignity In Dying. Let me state right away that I fully accept there are individuals who take this position; the same goes for people with significant impairments, but it is sheer arrogance to use their opinion as a generalised expression in order describe how everyone feels about their condition or situation.
The Disabled People’s Movement was never a voice for all disabled people; how could it be when it had a broad, yet specific, agenda: the emancipation of disabled people. [There are people who would prefer to be called crippled rather than being viewed as ‘disabled by society’.] The legitimising of disabled people’s social oppression is dominant ideology and culture based upon individualism and normality – body fascism – which sees ‘abnormality of the body’ as an individual personal tragedy. Stewart’s emotive language evokes the dominant cultural appraisals surrounding illness and impairment:death is a release from the lingering suffering of a screwed body; let’s be candid about what’s implied, for a change.
“I am not truly free if I am taking away someone else’s freedom, just as sure as I am not free when my humanity is taken from me. The oppressed and the oppressor alike are robbed of their humanity.” ~ Nelson Mandela
Preamble
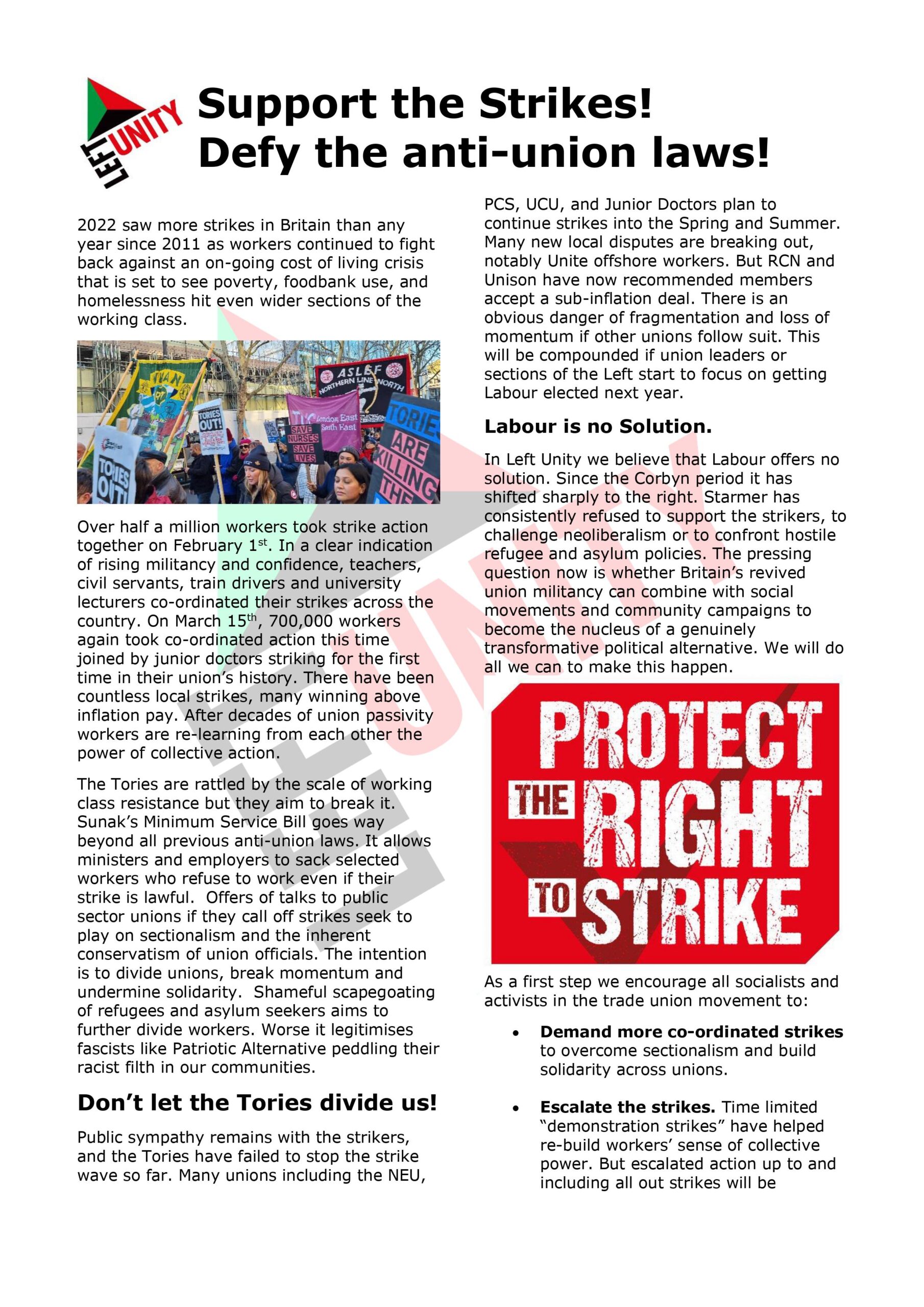
Left Unity recognises the need to address issues relating to Health and Social Policy within the context of the nature of the society in which we live. The discussions around assisted dying/suicide should not be reduced to addressing the needs of people with failing health or an assessment of what is judged to be a deterioration of a quality of life. This statement refers to the debate as being about ‘assisted dying/suicide’ because the meaning of the terminology employed is hotly contested.
A central part of any discussion of this issue must include how the nature of capitalist society impacts upon people’s individual autonomy and their freedom to make choices. It has to be acknowledged that the nature of society creates unequal and differential treatment for people with significant health conditions and impairments. How people with significant health conditions and impairments are both seen and treated within existing social relations creates the basis of their social oppression as disabled people. The main event in capitalist free markets is the creation of wealth. The other event is the creation of inequality. It is argued that where an individual finds him or herself in relation to the economic struggle for survival is dependent upon their abilities, intelligence or character; failure to succeed is laid squarely at the feet of the individual. Others legitimise inequality by arguing that it is part of ‘natural selection’ as defined by Social Darwinism which can be found within the historical development of eugenics. Why does the idea of ‘the survival of the fittest’ matter within today’s society?
In the current socio-economic climate there is a continued rightward swing of the pendulum. Attacks upon the National Health Service and the welfare state, the weakening of trade union power, coupled with an aggressive corporate culture and increased materialism all signal a formidable threat. People struggling for social justice have reason to fear because laissez faire capitalism and Social Darwinism are on the rise again. There are many sections of British society who have suffered as a direct consequence of the neoliberal agenda dressed up as ‘austerity measures’, however, particular attention needs to be paid to the vulnerable position of people with life-shortening impairments, chronic ill-health, those with significant impairments and older people find themselves in.
The Telegraph in 2008 quoted Baroness Warnock, who is considered an influential medical ethics expert, as saying “Elderly people suffering from dementia should consider ending their lives because they are a burden on the NHS and their families.” This is the exact same sentiment expressed in the Weimar Republic in Germany in the 1920s. It should also be noted that by 1938 the tide of public and official benevolence toward disabled people had begun to turn. The public mind now characterized disabled people as a separate, different, often criminalized group of less economic value than their non-disabled counterparts. The events of history weigh heavily upon the shoulders of disabled people because existing societal attitudes towards illness, impairment and old age continue to result in practice which marginalise, exclude and threaten those who are not perceived as having the same social and economic value as those deemed to be ‘fit and healthy’ with the ability to contribute to capitalist society.
Negative societal attitudes towards disabled people can be seen in various forms of legislation, for example, exclusion of disabled women from the Serious Crime Act 2015. This act extends the definition of domestic abuse to include psychological, emotional and financial coercion and control, but it excludes disabled women because of the difficulty of interpreting ‘carers’ interventions when presented as ‘in the best interests’ of the woman. Section 76 of the SCA puts the onus on the victim to prove that the abuser was not acting in her best interest, but clearly this is extremely difficult to do if she is living and obviously impossible if she were killed. Therefore disabled women have no protection against psychological, emotional or financial control/coercion and assisted suicide/dying could easily turn into murder and who would know? The possibility for hidden or unforeseen legal loopholes existing, which would permit abuse, are quite high because little legislation is ever scrapped and it is extremely difficult to screen out all ‘creative’ readings.
The contours of the current debate on assisted dying/suicide
During the Scottish Parliamentary debate on ‘Assisted Dying’ held on 28th May, 2015 Siobhan Mahon MSP stated, “It is not a medical condition that makes disabled people’s lives intolerable; it is the lack of social care, health services, accessible housing, transport and well-funded welfare benefits.” She went on to say that the bill “reinforces the stereotype that disabled people are a burden and do not contribute to society”, a stereotype that “could not be further from the truth and must not be given validity today, tomorrow or at any time in the future”.
The views expressed by Mahon are shared by many people who have concerns regarding the introduction of legislation in relation to ‘assisted dying/suicide’ however there are others who take an opposing stance. The central question should not be whether one is in favour or opposed to ‘assisted suicide’ but rather, what would be the implications and social consequences of passing legislation that would legalise a supported death? Consider the fact that within British society the notion of ‘human life’ becomes synonymous with “the human condition” which usually boils down to being about ‘normal people’ (sic). If this is so, then the idea of taking a human life is largely viewed as unacceptable, and this in turn paved the way for the social democratic-liberal opposition to the ‘death penalty’ and in some belief systems opposition to war. Where this becomes disrupted is when the people become ‘other than normal’, (sic) and as a consequence, they become gazed upon differently and their value and social worth becomes problematic.
Killing normal people is deemed to be murder whereas the killing of a non-normal person is often viewed as being ‘compassionate’ because it ends ‘suffering’. This would suggest ‘human life’ isn’t about people with terminal illnesses or significant impairment; the essence is judged to be missing and therefore the question of ‘an individual with/without pain’ isn’t the primary driver, but rather, lacking ‘human life’ constitutes the basis of perceived “suffering.” Consider too the implications that lie behind the legal system’s treatment of a mother who killed her three children with spinal muscular atrophy (a progressive weakening of the muscles over many years). Although found technically guilty, she was freed on ‘compassionate’ grounds even though the children were not ill: Prosecutor Zoe Johnson told a hearing at London’s Central Criminal Court that Clarence “Killed her three children because she wanted to end their suffering.”
This is however but one example of how the law currently discriminates against disabled people or values their lives differently. The arguments on both sides of the debate on assisted dying/suicide are commonly set out in the following manner:-
Supporters of legislation legalising assisted dying/suicide claim that all persons have a moral right to choose freely what they will do with their lives as long as they inflict no harm on others. This right of free choice includes the right to end one’s life when we choose. For most people, the right to end one’s life is a right they can easily exercise. But there are many who want to die, but whose disease, condition or impairment renders them unable to end their lives in a dignified manner. When such people ask for assistance in exercising their right to die, their wishes should be respected. Furthermore, it is argued, we ourselves have an obligation to relieve the suffering of our fellow human beings and to respect their dignity. Lying in our hospitals today are people with excruciatingly painful and terminal conditions and diseases that have left them permanently incapable of functioning in any dignified human fashion.
This is countered with the argument that:-
If assisted dying/suicide is allowed on the basis of mercy or compassion what will keep us from “assisting in” or actively urging, the death of anyone whose life we deem worthless or undesirable? And, once we accept that only life of a certain quality is worth living, where will we stop? When we devalue one life, we devalue all lives. Who will speak for those unable to speak for themselves? Finally, it is argued that sanctioning assisted suicide would violate the rights of others. Doctors and nurses might find themselves “pressured” to cooperate in a patient’s suicide. In order to satisfy the desires of a patient wanting to die, it’s unjust to demand that others go against their own deeply held convictions.
It is society that robs people of a ‘good death’, not illness. With proper pain medication and decent patient-centred palliative care, a ‘good death’ can be had. It’s never easy but it can be effectively managed to prevent unnecessary suffering. People will die in pain and distress unless the authorities ensure all terminally ill people get the palliative support they need.
There is however a third stance which suggests there are valid points and fundamental flaws in both sets of arguments which weaken the cases being presented and as a result makes resolution impossible. Where should Left Unity stand on this complex issue?
Understanding the debate
The debate around ‘assisted dying/suicide’ relies on a number of concepts and definitions some of which have been around for a considerable length of time and others which are either new or come from the re-shaping of older ones in order to explain new social contexts. A concept is an abstract idea which aids the way we make sense of something whereas a definition offers an exact meaning of a word or object. Let’s begin by considering our understanding of what is meant by suicide. The word comes from the Latin sui caedere which means “to kill oneself”. Thus suicide is regarded as being ‘the act of a human being intentionally causing his or her own death’. Immediately we are presented with the key feature: the role of an individual in the taking of their own life. Within the majority of Western cultures the notion of suicide is therefore an individualised act or is a shared act.
The House of Lords Select Committee on Medical Ethics has stated that the precise definition of euthanasia is “a deliberate intervention undertaken with the express intention of ending a life, to relieve intractable suffering.” http://en.wikipedia.org/wiki/Euthanasia – cite_note-Harris-2001-0#cite_note-Harris-2001-0. Here we have three elements working together:
- a deliberate intervention – an external act
- an express intention – the aim is to take a life
- to relieve intractable suffering – the “justification”
Of the three elements it is the final one that concerns us here. It has been called the “justification” because it acts as an attempt to make visible the reasoning behind the taking of an individual’s life and in so doing legitimate the act. The notion of ‘relieving intractable suffering’ lies at the heart of the debate. There are huge differences of opinion as to what “intractable suffering” means, not to mention the cultural values that are attached to it. The word intractable means: ‘hard to control or deal with’; therefore it is employed to signal the idea that the ‘possibility of managing the “suffering” by any alternative means is unlikely.’ Thus the word is being used to establish the grounds upon which the action – taking a life – can take place. It should be the final option as no other solution exists. How does the word “intractable” interact meaningfully given the different sets of opinion that surround what is meant by “suffering”? As a transitive verb, to suffer in every day English, means “experience or be subject to (something bad or unpleasant)” however as an intransitive verb it is often employed to denote being subjected to illness or impairment. In cultural terms how do we distinguish between “suffer from a cold” as opposed to “suffer from cerebral palsy” for example? Are we being invited to use common sense; rely on prior knowledge and understanding or perhaps it is a case of falling back upon subjective opinion?
How then does this impact upon our understanding of suffering? One interpretation relating to the law on euthanasia in relation to “intractable suffering” stated: “It deals specifically with the situation where someone is in great pain due to an illness or a disease”. Here ‘great pain’ is highlighted, but again, is this a shared understanding? There is a body of opinion that has a problem with applying the term “euthanasia” to the Action T4 programme because in their opinion, ‘euthanasia implies that the death is for the person’s direct benefit.’ Thus they argue what the Nazis did was to kill people without any consideration of benefit to the person killed and therefore it was straight forward murder. Could we question this interpretation? Given the dominant approach towards disability within many Western societies, ‘to have an existence rather than a life’, is often the way in which disabled people’s lives are viewed and often this alone is the reason why euthanasia is viewed as ‘benefiting the person’.
Is there a fundamental difference between euthanasia, ‘assisted suicide’ and ‘assisted dying’? Within current discourses the language becomes problematic.
The concepts and language employed
The concepts and language employed are often problematic and rely on euphemisms. Assisted suicide and euthanasia are sometimes combined under the umbrella term “assisted dying”, an example of a trend by advocates to replace the word “suicide” with “death” or ideally, “dying”. Other euphemisms in common use are “physician-assisted dying”, “physician-assisted death”, “aid in dying”, “death with dignity”, “dying with dignity”, “right to die” “compassionate death”, “compassionate dying”, “end-of-life choice”, and “medical assistance at the end of life”.
Physician-assisted suicide (PAS), involves a doctor “knowingly and intentionally providing a person with the knowledge or means or both required to commit suicide, including counselling about lethal doses of drugs, prescribing such lethal doses or supplying the drugs.
The array of euphemisms means it far from clear as to who would actually be covered by legislation on ‘assisted dying’. Those arguing for assisted suicide legislation say it is not about disabled people. In Britain the campaign group, Dignity in Dying, argue that there are only advocating a change in the law on assisted dying. This is where terminally ill adults who meet strict criteria and satisfy legal safeguards would have the option to take life-ending medication and die peacefully at home. They argue assisted dying and assisted suicide are not the same and there is a clear difference between helping someone to die who is terminally ill and helping someone to die who is not. Many question this assertion of a ‘clear difference’ because the existing the current proposals outlined in the ‘Assisted Dying Bill’ are based upon the Oregon model which legalised assisted suicide over ten years ago.
It is reported that doctors who write lethal prescriptions are required to supply certain after-the-fact data. While there is reason to question whether all of them do so, and the data being collected is minimal, a ten year statistical summary indicates that most of those who sought lethal prescriptions acted out of fear of future conditions, not worries over dying in pain. The “suffering” people reportedly sought to avoid by committing suicide involved anticipated loss of “dignity” and “autonomy”, the prospect of losing control of bodily functions and needing personal care, and worries over the “burden” that continuing to live might place on others. Dignity in Dying, continue to argue that their Bill is only to cover ‘terminally ill adults who meet strict criteria and satisfy legal safeguards’ however if it is based upon the Oregon model, there remains serious questions to be asked. It is argued by opponents of legislation that definitions of ‘terminal illness’ can never be precise and they cite the fact people with Multiple Sclerosis are disabled people and yet they are the people targeted most frequently as beneficiaries of assisted suicide legislation.
Concepts such as the ‘right to live’, the ‘right to choose’ and the ‘right to die’, are employed in a range of debates concerned with individual rights. The concept of a right to life is central to debates on the issues of capital punishment, war, abortion, euthanasia and justifiable homicide. The entitlement of a person to make the decision to end their own life through euthanasia is commonly called a right to choose, whereas opposition to legalisation on euthanasia and assisted suicide is commonly framed in terms of the right-to-life. However the term “right to life” is also used in the abortion debate by those who wish to outlaw the intentional termination of a pregnancy and the term “right to choose” is employed by those who defend the right of a woman to have an abortion. It should also be noted there is no legal ‘right to die’ within Human Rights law and therefore much of the debate on the issues connected with ‘the right to die’ tend to be played out within religious or moral contexts.
Are there double standards at work?
Can we accept the premise that the current debate on introducing legislation in relation to ‘assisted dying’ is limited solely to those people defined by Lord Falconer and Dignity in Dying’? The grounds of debate keep shifting. Within the ranks of the lobby who want legislation are those who would advocate that assisted dying/suicide gives the same opportunity to take actions open to fully functional individuals; however it is necessary to question what this means in reality. The concept often referred to is a ‘right to choose’ however what is the relationship between having a desire to carry out a specific act and the actual ability to fulfil that desire? Within dominant discourses relating to individual choice this is almost always reduced to the question of functional ability and for those lacking various degrees of functional ability these discourses tend to produce oppressive consequences. It is at this point that it is necessary to explain why advocates of the social model of disability make a clear distinction between issues surrounding illnesses and impairments and issues relating to disability which is defined as the experience of social restrictions. This model explores the how and why social restrictions are ‘imposed on top of our impairments’ – in other words, social barriers that go beyond the functional incapacity caused by our conditions. It is acknowledged that there are restrictions of functioning directly caused by the realities of impairment and no amount of ‘adjusting’ of the social environment will alter their impact. The experience of disability, however, arises when the realities of impairment can or could be addressed within social contexts but are not. Where the ability to socially interact is denied or restricted this should be understood as a site of disablement. It should also be acknowledged that when addressing the issue of disablement we should start from the ways oppression differentially impacts on different groups of disabled people rather than with differences in experience among individuals with different impairments. This approach is often absent within the debates surrounding assisted dying/suicide. Those who believe in equality for disabled people should not ignore ‘the reality of impairment’ because this is often the reason why disabled people are subjected to unequal and differential treatment resulting in social oppression. Nevertheless, the reality of impairment needs to be contextualised not assumed.
Why raise this issue within the context of the assisted dying/suicide debate? It is often argued that the ‘right to die’ is based upon the premise that: ‘… if people who have full functioning bodies can commit suicide, so why shouldn’t people who lack this functional ability have help to do it?’ Can this question be posed and answered in isolation? What relation does this question have in the context of the question disabled people have been asking for decades: ‘… if people who have full functioning bodies can live independently within society, so why shouldn’t people who lack specific forms functional ability have help to do it?’ What is so ‘special’ about this action – taking one’s own life – that places it above millions of other functional acts that exist? We are told, this is a “special” case because people should not be forced to endure ‘pain and suffering’ or forced to live lives that are lacking in quality. Exactly who is it that is deciding where to draw the boundaries around what constitutes ‘pain and suffering’ or lives that lack quality? The current debate around assisted dying/suicide collapses together the ‘quality of life’ expected or accepted of a ‘healthy’ human being and the state of being of people who are ill, with terminal illness or significantly impaired. It is the use of societal comparators that makes the debate oppressive and, many would argue, unsafe to legislate. Where a society maintains a binary approach – prolong life or end suffering – there’s historical evidence to suggest that this ultimately results in coercive practices when subjectively applied to ‘groups of people’ across the board.
In questioning the premise on which the case for supporting assisted dying/suicide is based, the aim is not to construct a dog in a manger argument, but rather to highlight the existence of double standards within capitalist society’s treatment of different groups of people. It is necessary to question why it is that there appears to be greater support for ‘the right to die’ than there is for ‘the right to live’. This has nothing to do with a ‘right to chose’ if such a right does not exist. There are people who have ‘elected to die’ simply because they were being denied access to opportunities which would have improved their quality of life. There have been disabled people and others with life-shortening illnesses for have taken their own lives as a result of benefit sanctions, fear of re-assessment in relation to their support needs and being forced back into unsafe and discriminatory labour market. It has to be remembered that we have a Government that refuses to publish the figures relating to people who have committed suicide or died after benefits were withdrawn or under review, despite requests under the Freedom of Information Act. It is necessary to ask: are these people’s stories appearing within the mass media on the same scale of those who publicly argue for ‘the right to die’ or propagate tales about ‘lazy disabled people’ on benefits?
Within Article Three of the UN Convention on the Rights of Persons with Disabilities, it states that the principles of the present Convention shall be:
- Respect for inherent dignity, individual autonomy including the freedom to make one’s own choices, and independence of persons;
- Non-discrimination;
- Full and effective participation and inclusion in society;
- Respect for difference and acceptance of persons with disabilities as part of human diversity and humanity;
- Equality of opportunity;
- Accessibility;
- Equality between men and women;
- Respect for the evolving capacities of children with disabilities and respect for the right of children with disabilities to preserve their identities.
We believe these eight principles should inform the policies and practice of Left Unity. In adopting these principles we recognise that Left Unity and its membership will be confronting and needing to challenge oppressive attitudes and practice which undermine and actively work against these principles. A central aspect of disabled people’s social oppression is the many ways in which they are denied both choice and control over their lives as a direct result of discriminatory attitudes which maintain and reinforce disabling barriers within the structures, systems and cultural values of capitalist society.
Disabled people have sought to challenge the material conditions of their oppression by raising the demand for ‘independent living’; creating the means whereby all disabled people can exercise the same freedom, choice, dignity and control as other citizens at home, a work and in the community. Independent living is based upon the right to practical assistance and support to participate in society and live an ordinary life. The policies introduced by the coalition government; the closing of the Independent Living Fund, cuts to, and the marketisation of, support services are a direct attack upon disabled people’s right to independent living and, as a consequence, the quality of life that they lead. The idea that people are living ‘too long’ and we can’t afford to care for them is gaining greater purchase. The Utilitarian argument that the needs of the many outweigh the needs of the few has been increasingly used against the interests of disabled and elderly people. This argument needs to be demolished.
What is largely absent from the debates around assisted dying/suicide is any acknowledgement of existing end of life support that is available to people who are terminally ill. Palliative care is defined as: “the active, holistic care of patients with advanced progressive illness. Management of pain and other symptoms and provision of psychological, social and spiritual support is paramount. The goal of palliative care is to achieve the best quality of life for patients and their families. Many aspects of palliative care are also applicable earlier in the course of the illness in conjunction with other treatments”. More latterly the importance of “early identification and impeccable assessment” has been added to this definition.
Principles of Quality Palliative Care
Good palliative care:
- is applicable from diagnosis;
- affirms life and regards dying as a normal process;
- seeks neither to hasten nor to postpone death;
- integrates the psychological, emotional and spiritual aspects of care;
- offers a support system to help people live as actively as possible until death;
- provides relief from pain and other distressing symptoms;
- offers a support system to help the family cope during a person’s illness ,death and bereavement;
- uses team approach to address the needs of people with advanced progressive illness and their families
- will enhance quality of life
Left Unity stance on assisted suicide, individual autonomy, and freedom of choice
Left Unity, acting within the principle of ‘respect for inherent dignity, individual autonomy including the freedom to make one’s own choices, and independence of persons’, believes individual autonomy should contain the right where possible for an individual to determine the quality of life they wish to live free of external pressures to extend or end that life. How ‘the quality of life’ is currently perceived within the field of healthcare is in terms of how it is negatively affected, on an individual level, a debilitating weakness that is not life-threatening, life-threatening illness that is not terminal, terminal illness, the predictable, natural decline in the health of an elder, an unforeseen mental/physical decline of a loved one, chronic, end-stage disease processes. Left Unity acknowledges that some individuals due to the nature of their illness or impairment may lack the ability to self-determine their own quality of life. Further, Left Unity believes that the people who find themselves within this vulnerable situation have, generally speaking, found their needs and interests excluded from the majority of discussions and proposed policies and legislation. Left Unity is committed to defending their rights and declares it is not in favour of either the state or society deciding on behalf of an individual what should determine their ‘quality of life’.
An area where choice and control can intersect with individual autonomy is what was known as making ‘a living will’. A ‘living will’ is the old name for an Advance Decision. An Advance Decision is the legal name for a document that allows a person to make a legally binding refusal of treatment in advance of a time when they cannot communicate their wishes, or do not have the capacity to make a decision. An Advance Decision can be used to refuse any treatment, including life-sustaining treatment such as resuscitation, artificial nutrition and hydration, and breathing machines. In October 2007 the Mental Capacity Act (2005) came into force and gave Advance Decisions a legal footing. One of the arguments strongly articulated at this current moment in time against legislating on assisted suicide is the belief that the state can’t be trusted to make the correct ‘safeguards’. Such concerns cannot be ignored, however the fear as to what a government might or might not do, should not be the determining factor in deciding what is an appropriate course of action.
Developing an alternative perspective
A major barrier to developing a principled position is that we are dealing with a variety of agendas; many of which are not transparent, or working in the interests of all people who could be affected by legislation on assisted dying/suicide. The legal position within existing law was clarified by the European Court of Human Rights which found that the right to life does not create an entitlement to choose death rather than life. As a consequence there is no right to die at the hands of a third person or with the assistance of a public authority. This is the position those in favour of assisted suicide wish to overturn. Left Unity recognises the debate around assisted dying/suicide is complex and is driven by conflicting interests which means a resolution cannot be easily be resolved. It is our belief that only by defending individual autonomy, fighting inequality, promoting dignity and respect, within the context of an anti-capitalist transformation of society, can the conditions for creating independent living and individual freedom of choice be fully realised.
Left Unity not only believes that in the current social context in which this debate is taking place, the case to change our current law has not been made, we also believe permitting assisted dying/suicide without the guaranteed ability of ensuring choice and control by the individual at all times could put vulnerable people at risk of harm.
Based upon this recognition Left Unity:
- must nevertheless champion individual autonomy including the freedom to make one’s own choices however it should be noted that an autonomous decision is not merely a wish, but a decision made with appropriate information and rational consideration of the outcomes.
- challenge the neoliberal agenda which undermines people’s civil and human rights. Within this challenge;
- articulate the impact the austerity measures have had on those who rely on the National Health Service and Welfare State
- continue to attack the demonisation of people on benefits who are unable to work
- oppose the increasing restrictions being placed upon disabled and elderly people’s ability to live independent lives
- oppose any state interference and individual interference or coercion which would take away people’s choices in relation to their individual autonomy.
- must oppose the use of forced medication and life support upon individual who have elected to end their life.
- believes the right to individual autonomy includes control over their own bodies and not to have the state or economic system determine completely those choices.
- believes that there should be an increase in resources within palliative care which allows patients to die with dignity; which would include support for an extension of hospice facilities and the offer of the possibility of dying at home to those who wish to choose that option. This provides support (physical and psychological) to die a natural death.
- believes that there are people who do not want to continue to live in various circumstances and their will must be respected.
- believes we should not force people to live when they do not want to do so on the grounds that such an act takes away the individual’s right to self-determination.
- believes individuals should have every right to choose to input into the manner of their death, for example, the use of a ‘Do Not Resuscitate’ notice or the deployment of an advanced decision.
- believes individuals have the right to say they do not want extraordinary measures carried out to keep them alive. Similarly, those that do want such measures should have the right to have them.
- believes doctors should never be forced to take a life, as this would make murderers of them, but asking them to withhold extraordinary measures is reasonable if conducted in a compassionate manner.
1 comment
One response to “Draft policy statement on assisted dying/suicide, individual autonomy and the freedom to make choices”
Left Unity is active in movements and campaigns across the left, working to create an alternative to the main political parties.
About Left Unity
Read our manifesto
Left Unity is a member of the European Left Party. ![]()
Read the European Left Manifesto
ACTIVIST CALENDAR
Events and protests from around the movement, and local Left Unity meetings.
ongoing
Just Stop Oil – Slow Marches
Slow marches are still legal (so LOW RISK of arrest), and are extremely effective. The plan is to keep up the pressure on this ecocidal government to stop all new fossil fuel licences.
Saturday 27th April: national march for Palestine
National demonstration.
Ceasefire NOW! Stop the Genocide in Gaza: Assemble 12 noon Central London
Full details to follow
More events »
GET UPDATES
Sign up to the Left Unity email newsletter.
CAMPAIGNING MATERIALS
Get the latest Left Unity resources.
I wish there were a clearer and stronger statement of opposition to legalizing assisted suicide beyond “Left Unity not only believes that in the current social context in which this debate is taking place, the case to change our current law has not been made, we also believe permitting assisted dying/suicide without the guaranteed ability of ensuring choice and control by the individual at all times could put vulnerable people at risk of harm.” It’s mushy.